Is your team leading AI or absorbing avoidable risk?
Executive Summary: Artificial intelligence has moved from the lab to operational reality in mental health (MH) and behavioral health (BH), and to the front lines of Call Centers (CC)! By 2025–2026, physician and health system adoption accelerated sharply, especially in documentation, administrative support, and workflow optimization. Federal agencies, including Health and Human Services, Veterans Affairs, Defense Health Agency, and Centers for Medicare & Medicaid Services, are building governance while scaling practical tools. The evidence is strongest for low-to-moderate-risk applications such as ambient documentation, scheduling, quality assurance, and structured follow-up. The leadership imperative is direct: deploy AI where it reduces friction, preserves human judgment, and strengthens operational capacity before attempting high-risk autonomous care.
AI Has Left the Lab. Operational Reality Just Changed
The strongest measurable returns are not autonomous diagnosis or robotic psychotherapy. They are operational. Ambient documentation reduces administrative burden. Scheduling automation improves access. Quality assurance tools improve consistency. Structured follow-up strengthens continuity.
In mental health, behavioral health, and crisis systems, evidence still favors augmentation over substitution. AI can support clinicians. It cannot safely replace them in high-risk moments involving crisis triage, vulnerable populations, or urgent psychiatric judgment.
According to JAMA, the current state of artificial intelligence (AI) is no longer defined by distant pilots. By 2025, AI use reached 8.3%; the sharpest increase occurred in outpatient and ambulatory settings. AMA’s reports: early 2026, 81% of surveyed physicians reported using augmented intelligence in practice, largely for documentation, summarization, and administrative support rather than autonomous diagnosis.
The most widely scaled near-term applications in mental health (MH), behavioral health (BH), and healthcare customer service and call center (CS/CC) operations are ambient documentation, patient access automation, portal message drafting, training and quality assurance, referral and scheduling support, and structured follow-up.
The real issue is no longer whether AI is coming; it’s whether it’s coming. It is whether leadership is disciplined enough to govern it.
Federal Health Systems Are Moving Out Deliberately
Major federal systems are not sprinting blindly. They are building governance structures, strategic frameworks, and targeted use cases. Health and Human Services, Veterans Affairs, the Defense Health Agency, and the Centers for Medicare & Medicaid Services now signal that AI belongs in strategic modernization, but within controlled boundaries.
The Department of Health and Human Services (DHHS) has expanded its AI use-case inventory and governance structures and recently published a National AI Strategy. The Department of Veterans Affairs (VA) is scaling selected high-impact tools such as AI-supported crisis-line training support and a broader enterprise AI strategy.
The Defense Health Agency (DHA) has laid the foundation for AI and is emphasizing digital transformation, AI governance, and responsible adoption with its 2026-2030 Data Strategy.
This effort matters. When federal systems move deliberately, the private and nonprofit sectors should pay attention. The message is practical: governance before scale, infrastructure before hype, accountability before automation. In fact, according to Psychiatry Online, the Centers for Medicare & Medicaid Services (CMS) has issued AI guidance and expanded payment pathways for digital mental health treatment.
Adoption alone means little if leaders misunderstand where AI actually works best.
The Biggest Wins Are Boring. That’s Good News
The strongest measurable returns are not autonomous diagnosis or robotic psychotherapy. They are operational. Ambient documentation reduces administrative burden. Scheduling automation improves access. Quality assurance tools improve consistency. Structured follow-up strengthens continuity.
JAMA reported Ambient AI documentation has been associated with lower EHR time, lower burnout, and modest financial gains, but raises concerns about coding intensity and spending growth. In BH, one randomized clinical trial by Eleos Health, which supported therapy documentation, measurement, and evidence-based feedback, found higher attendance, greater symptom reduction, and faster note completion than treatment as usual.
In mental health, behavioral health, and crisis systems, evidence still favors augmentation over substitution. AI can support clinicians. It cannot safely replace them in high-risk moments involving crisis triage, vulnerable populations, or urgent psychiatric judgment.
The Journal of Medical Research Journal reports that machine learning (ML) in crisis call center services has shown potential for scalable quality monitoring of suicide risk assessment in counseling calls and for acoustic-feature detection of suicide risk. However, published evidence does not fully support the use of autonomous crisis triage. The 988 Suicide & Crisis Lifeline’s launch has been associated with lower youth suicide mortality, but that gain reflects system expansion and human crisis infrastructure.
According to Stanford, studies indicate there is no hard evidence that conversational AI can safely replace clinicians or crisis counselors. This observation shows how poor leadership causes preventable harm. Black-box automation in sensitive care settings can introduce legal, ethical, and operational failures.
The Implications For Leadership Teams Are Straightforward
Use AI first where it reduces friction, not where it substitutes for professional judgment. Smart leaders use AI to reduce friction, not replace judgment. The table below summarizes the challenges:

In MH, BH, and CS/CCs, the highest-confidence near-term investments are documentation, CSR assist, scheduling-referral automation, outreach and follow-up, structured QA, and population management.
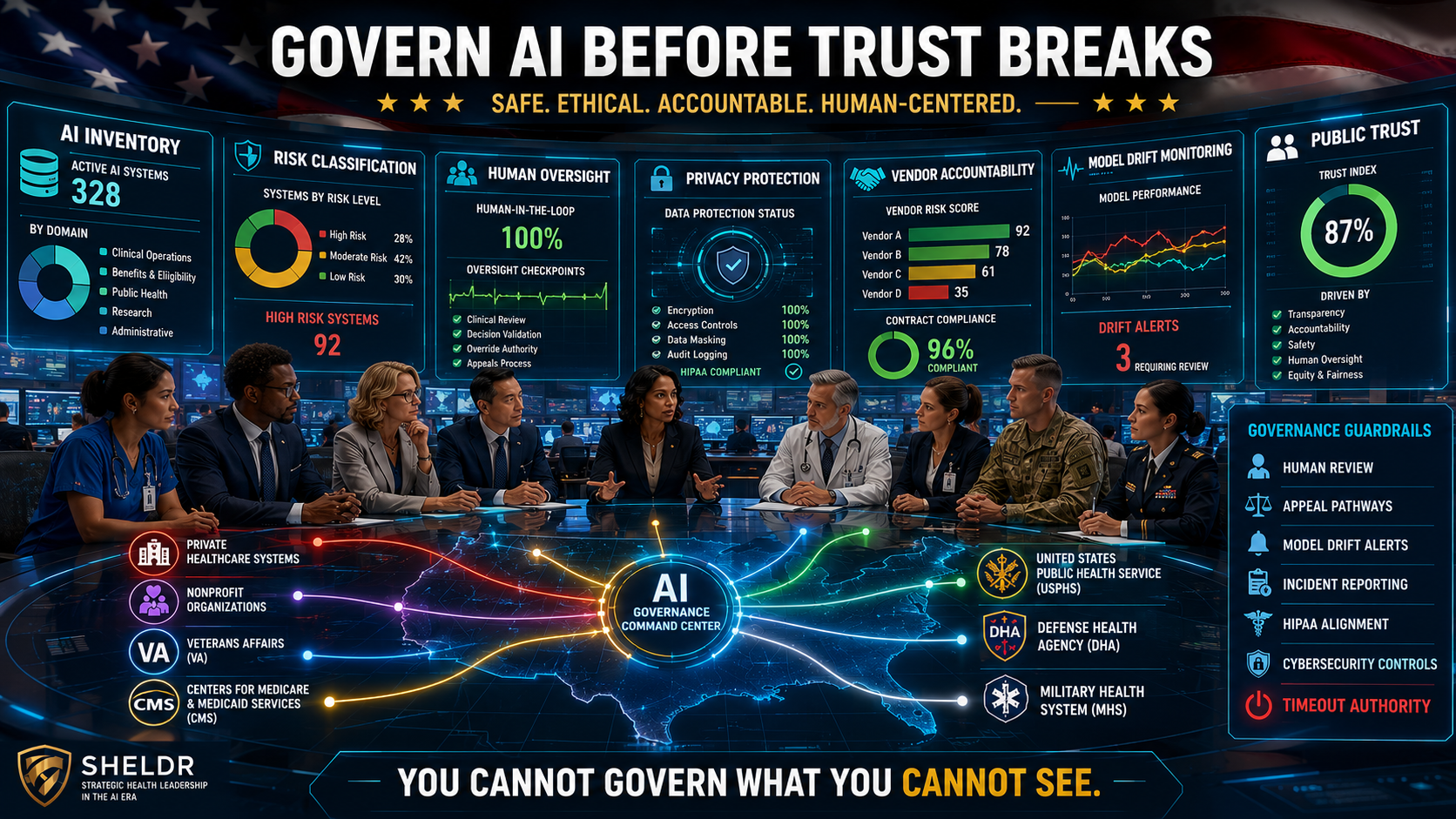
Governance is your real competitive edge. Governance, such as IBM’s framework, must therefore come before scale: local validation, data and model inventory, auditability, monitoring for drift and bias, disclosure rules, human-in-the-loop design, and explicit stop authority. Before expanding AI, leadership teams need 7 brutal AI non-negotiables:
- Local validation
- Data and model inventory
- Auditability
- Drift and bias monitoring
- Human-in-the-loop design
- Disclosure protocols
- Explicit TIMEOUT AUTHORITY
AI failure rarely starts with technology. It usually starts with leadership skipping governance because speed feels more exciting than discipline. Before you act, get the basics right.
Conclusion and Call to Action
AI is already embedded in modern health operations. The question is not whether organizations should engage, but whether leaders will do so strategically or recklessly. Current evidence supports AI as a force multiplier for operational efficiency, documentation, and access, not autonomous high-risk care. Health leaders must prioritize governance, accountability, and phased implementation over hype. Start with low-risk workflow gains, define boundaries, and build trust before scaling.
Move now, but move intelligently. Delay creates risk. Poor governance multiplies it.
Discussion Questions
- Where is your organization currently using AI, formally or informally?
- Which low-risk workflows could generate immediate value without compromising judgment?
- Does your organization have clear AI governance, audit, and TIMEOUT AUTHORITY policies?
- What high-risk AI applications should be delayed until stronger evidence exists?
- Are your leaders treating AI as a strategy, a compliance issue, a workforce redesign, or all three?
Learn more: AI Tools: 3 Proven Steps to Selecting The Best For Your Use- IDOTS